Ulcerative Colitis: causes, symptoms, treatment, prevention: Stress and diet misfires trigger up to 50% of flare-ups
Understanding what is ulcerative colitis, its diverse symptoms of ulcerative colitis, potential causes, strategies for prevention of flares, and comprehensive treatment and management options is crucial for those living with the condition. This guide will delve into these aspects, explain how is ulcerative colitis diagnosed, and highlight how modern teleconsultation platforms like MaNaDr can provide vital support.
1. What Is Ulcerative Colitis
To truly understand this complex condition, it’s important to grasp the fundamental ulcerative colitis definition and what makes it distinct from other digestive issues. Often referred to simply as UC (the uc medical abbreviation), it is a specific type of inflammatory bowel disease.
1.1. Ulcerative Colitis Definition and Meaning
Ulcerative colitis is a chronic inflammatory bowel disease (IBD) that primarily affects the large intestine (colon) and the rectum. The ulcerative colitis disease is characterized by continuous inflammation that starts in the rectum and extends upwards into the colon. This inflammation causes tiny sores, or ulcerative colitis ulcers, to develop on the lining of the colon, which can bleed and produce pus.
For those asking, “what is ulcerative colitis” or “what is uc,” it’s a condition where the immune system mistakenly attacks the digestive tract, leading to chronic inflammation and damage. Unlike Crohn’s disease (another form of IBD), ulcerative colitis affects only the colon and rectum, and the inflammation is continuous, not patchy. Understanding the ulcerative nature of this ulcerative colitis is key to recognizing its symptoms.
1.2. How Common is Ulcerative Colitis? (Prevalence & Impact)
Ulcerative colitis is a significant public health concern globally. It affects millions worldwide, with its prevalence steadily increasing in many regions.
In North America, it’s estimated that approximately 1 million people live with IBD, with a substantial portion having ulcerative colitis (Crohn’s & Colitis Foundation). Globally, the incidence and prevalence of IBD, includingulcerative colitis, have been rising, particularly in newly industrialized countries.
Ulcerative colitis can develop at any age, but it is most commonly diagnosed in individuals between the ages of 15 and 30, and sometimes in people over 60.
Once diagnosed, ulcerative colitis is a chronic condition that requires lifelong management. Its impact extends beyond physical symptoms, profoundly affecting an individual’s quality of life. Patients often experience unpredictable flare-ups, leading to disruptions in work, school, social activities, and overall well-being. This can lead to anxiety, depression, and significant challenges in daily living.
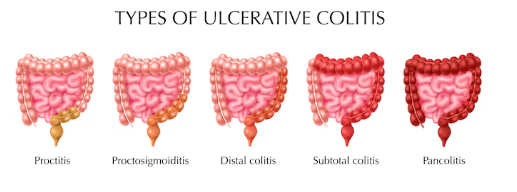
1.3. Types of Ulcerative Colitis
The manifestation of UC varies significantly depending on how much of the colon is affected by inflammation. This progression of inflammation defines different patterns of the disease, each with its own set of characteristics and typical symptom profiles:
Ulcerative Proctitis: In this form, inflammation is confined solely to the rectum, which is the final section of the large intestine. It’s often considered the mildest presentation of UC.
Proctosigmoiditis: Here, the inflammation extends beyond the rectum to also involve the sigmoid colon, which is the S-shaped lower part of the colon.
Left-Sided Colitis: This pattern describes inflammation that begins in the rectum and spreads continuously upwards, affecting the descending colon and often reaching the splenic flexure (the bend in the colon near the spleen). Individuals with this type often experience descending colon pain.
Pancolitis: This is the most extensive form of UC, where inflammation affects the entire colon, from the rectum all the way through to the cecum. It’s often associated with more severe symptoms and a higher risk of complications.
1.4. Expert Insight: UC vs. IBS
Expert Insight: A common myth is that “Ulcerative Colitis is just a more severe type of Irritable Bowel Syndrome (IBS).” However, leading gastroenterologists and organizations like the Crohn’s & Colitis Foundation emphasize the crucial fact that Ulcerative Colitis is a serious, chronic inflammatory bowel disease (IBD) involving actual inflammation, ulcers, and damage to the colon lining. This is fundamentally different from IBS, which is a functional gastrointestinal disorder without inflammation or structural damage to the bowel. While both conditions share some symptoms like abdominal pain and changes in bowel habits, their underlying pathology, diagnostic methods, and treatments are distinct.
2. What Are the Symptoms and Signs of Ulcerative Colitis?
The signs and symptoms of ulcerative colitis can vary widely among individuals, depending on the severity of inflammation and how much of the colon is affected. These ulcerative colitis symptoms often appear gradually and tend to come in cycles of flare-ups (active disease) and periods of remission (when symptoms are minimal or absent). Understanding what are the symptoms of ulcerative colitis is crucial for early recognition.
2.1. Overview of UC Symptoms
Recognizing the patterns of uc symptoms is key, as they directly reflect the inflammation in the colon. These symptoms can range from mild to severe, and they significantly impact daily life during a flare-up.
2.2. Common Gastrointestinal Symptoms
The most prominent ulcerative colitis symptoms are related to the digestive tract:
Bloody Diarrhea: This is the most common symptom, often accompanied by pus or mucus. The amount of blood in ulcerative colitis poop or ulcerative colitis stool can vary from streaks to significant bleeding.
Abdominal Pain and Cramping: Discomfort in the abdomen, which can range from mild to severe. The specific ulcerative colitis pain location can vary depending on where the inflammation is, often felt in the lower abdomen.
Urgency to Defecate: A sudden, strong, and often uncontrollable urge to have a bowel movement, sometimes leading to accidents.
Tenesmus: A feeling of incomplete bowel evacuation, even immediately after a bowel movement, leading to straining.
Rectal Pain: Discomfort or pain in the rectal area, especially if the inflammation is confined to the rectum (proctitis).
Weight Loss: Due to chronic inflammation, poor nutrient absorption, and decreased appetite during flares.
Fatigue: Persistent tiredness and low energy, often a result of chronic inflammation, pain, and sleep disturbance.
Anemia: Blood loss from the colon can lead to iron-deficiency anemia, causing fatigue and weakness.
2.3. Extraintestinal Manifestations (Symptoms Outside the Gut)
Ulcerative colitis can also cause symptoms that affect other parts of the body, known as extraintestinal manifestations. These occur in approximately 25-40% of individuals with IBD:
Joint Pain (Arthritis): Inflammation and pain in the joints, most commonly affecting large joints like the knees, ankles, and hips.
Skin Lesions: Various skin problems, including painful sores (pyoderma gangrenosum) or tender red nodules (erythema nodosum) that usually appear on the legs.
Eye Inflammation: Conditions like uveitis (inflammation of the middle layer of the eye) or episcleritis (inflammation of the white part of the eye), leading to redness, pain, and sensitivity to light.
Liver Disorders: Though less common, UC can be associated with certain liver and bile duct problems, such as primary sclerosing cholangitis (PSC).
2.4. Ulcerative Colitis Complications
If left unmanaged or during severe flares, ulcerative colitis can lead to serious complications. Recognizing these is vital for timely medical intervention:
Toxic Megacolon: A rare but life-threatening complication where severe inflammation causes the colon to rapidly expand and swell. Symptoms include severe abdominal pain, fever, rapid heart rate, and dehydration, requiring immediate medical attention.
Colon Cancer Risk: Individuals with ulcerative colitis, especially those with extensive disease or a long duration of illness, have an increased risk of developing colorectal cancer. Regular screening colonoscopies are crucial for early detection.
Severe Bleeding: Chronic inflammation and ulcers can lead to significant blood loss, worsening anemia, and potentially requiring blood transfusions.
Perforation of the Colon: In rare, severe cases, the inflamed colon wall can thin and tear, leading to a perforation (hole) that allows bowel contents to leak into the abdominal cavity, causing a life-threatening infection (peritonitis).
Strictures: While more common in Crohn’s, repeated inflammation can sometimes lead to narrowing of the colon (strictures), which can obstruct the passage of stool.
Malnutrition and Growth Failure: Especially in severe, chronic cases, poor absorption of nutrients due to inflammation and chronic diarrhea can lead to malnutrition and, in children, growth failure.
2.5. Gender-Specific Considerations in Symptoms
While the overall prevalence of ulcerative colitis is generally considered to be similar between males and females, the experience of ulcerative colitis symptoms in females can have unique considerations due to biological differences:
Menstruation: Many females with UC report that their gastrointestinal symptoms, such as diarrhea, abdominal pain, and urgency, tend to worsen during menstruation due to hormonal fluctuations.
Pregnancy and Fertility: UC can impact fertility for some individuals, though many women with UC are able to conceive. Managing the condition during pregnancy requires careful planning with a gastroenterologist and obstetrician to ensure both maternal and fetal well-being, as disease activity can fluctuate during gestation.
Pelvic Floor Dysfunction: Chronic diarrhea and urgency can sometimes lead to pelvic floor muscle weakness or dysfunction, which might exacerbate symptoms like fecal incontinence or rectal pain, more commonly affecting females.
Sexual Health: Pain and fatigue from UC can impact sexual health and intimacy, an aspect that may be particularly challenging for females.
If you are experiencing persistent digestive symptoms or suspect you might have ulcerative colitis, and are seeking clarity, MaNaDr offers a discreet way to consult with online doctors 24/7 to discuss your concerns and get guidance on next steps.
3. What Causes Ulcerative Colitis?
Understanding what causes ulcerative colitis is complex, as the exact etiology remains unknown. However, research points to a multifactorial interplay of genetics, immune system dysfunction, and environmental triggers. This helps address reasons for ulcerative colitis and shed light on how do you get ulcerative colitis.
3.1. Underlying Causes: Immune System and Genetics
While there isn’t a single definitive cause for ulcerative colitis, several fundamental factors are believed to initiate its development:
Immune System Dysfunction: The most widely accepted theory suggests that ulcerative colitis is an autoimmune disease. In individuals with UC, the immune system mistakenly identifies harmless bacteria, food, or other substances in the gut as foreign invaders. This leads to a chronic inflammatory response that damages the lining of the colon and rectum, creating ulcerative colitis ulcers.
Genetics: A strong genetic predisposition exists. Individuals with a family history of ulcerative colitis or Crohn’s disease (IBD UC) are at a higher risk of developing the condition. While it’s not inherited in a simple Mendelian fashion, many genes have been identified that are associated with an increased risk.
3.2. Risk Factors
Beyond the direct underlying causes, several factors are considered risk factors that can either increase an individual’s susceptibility to developing ulcerative colitis or, more commonly, trigger its flare-ups in those already predisposed. Understanding what causes uc flare-ups often involves these elements.
Family History: Having a close relative (parent, sibling, child) with UC or Crohn’s disease significantly increases your risk, reinforcing the genetic component.
Ethnicity: People of Ashkenazi Jewish descent have a higher risk of developing UC. The condition is also more common in white populations, though incidence is rising in other ethnic groups globally.
Age: While UC can occur at any age, diagnosis most commonly happens between 15 and 30 years old, or occasionally in individuals over 60.
Geographic Location: UC is more prevalent in developed countries and urban areas compared to developing countries and rural areas, suggesting environmental influences related to Western lifestyles.
Smoking Status: Interestingly, smoking is a significant risk factor for Crohn’s disease, but for ulcerative colitis, current smokers have a lower risk of developing the disease. However, quitting smoking can paradoxically trigger UC symptoms in former smokers. Despite this, quitting is always recommended for overall health.
Dietary Triggers: While diet does not cause ulcerative colitis, certain foods are widely recognized as significant triggers for symptom flare-ups in many individuals. High-fat foods, dairy, high-fiber foods (during flares), spicy foods, and caffeine can worsen colitis sintomas.
Stress: As the article title highlights, while stress does not causeulcerative colitis, it is a widely recognized and significant trigger for ulcerative colitis flare-ups. Stress can exacerbate inflammation and impact gut function.
Medications: Some medications, particularly Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) and antibiotics, are not causes of UC but can sometimes trigger or worsen flare-ups in individuals with the condition.
3.3. Other Contributing Factors
Beyond the primary causes and established risk factors, other elements are being explored in the etiology of ulcerative colitis:
Gut Microbiome: Imbalances in the trillions of bacteria living in the gut (the microbiome) are thought to play a crucial role in perpetuating chronic inflammation in UC. Research suggests a dysbiosis (imbalance) in the gut flora could contribute to the immune system’s abnormal response.
Infections: Some theories suggest that certain bacterial or viral infections might trigger the initial immune response in genetically predisposed individuals, setting off the autoimmune cascade.
3.4. Expert Insight: UC is Not Contagious
Expert Insight: A common myth is that “Ulcerative Colitis is simply an infection you can catch from someone or that it’s contagious.” The crucial fact is that UC is a complex chronic autoimmune disease where the body’s immune system mistakenly attacks its own colon. It is not contagious and cannot be “caught” from another person like a cold, flu, or other infections. It’s a condition arising from internal biological predispositions and environmental interactions, not external transmission.
4. How Can Ulcerative Colitis Be Prevented?
For those living with ulcerative colitis or concerned about developing it, the question of “How can Ulcerative Colitis be prevented?” is paramount. Given its complex causes, prevention focuses on different aspects.
4.1. Prevention of Onset (Current Understanding)
Currently, there is no known way to prevent the initial onset of ulcerative colitis. Due to its complex, multifactorial etiology involving genetics and immune system dysfunction, scientists have not yet identified a definitive preventative measure that guarantees an individual will not develop the condition. Research is ongoing into potential early life factors that might influence risk, but at present, there are no specific actions that can reliably prevent someone from getting UC.
4.2. Preventing Flare-ups and Complications
While preventing the disease itself is not yet possible, management strategies are highly effective at preventing or reducing the frequency and severity of ulcerative colitis flare-ups and complications. This is where active “prevention” focuses for those with the condition:
Medication Adherence: This is the single most important strategy for maintaining remission and preventing flares. Consistently taking prescribed ulcerative colitis medications as directed, even when feeling well, is crucial to keep inflammation under control.
Dietary Management: While no specific diet causes UC, identifying and avoiding personal trigger foods can significantly help manage symptoms and prevent flares. Many individuals find relief with individualized dietary approaches, such as low-residue or low-FODMAP diets, especially during active flares. Keeping a food diary can help pinpoint specific sensitivities.
Stress Management: As noted, stress is a common trigger for ulcerative colitis flare-ups. Incorporating stress-reduction techniques like mindfulness meditation, yoga, regular exercise, adequate sleep, and seeking therapy can be highly beneficial in managing the disease’s course.
Avoiding NSAIDs (Nonsteroidal Anti-Inflammatory Drugs): For some individuals with UC, NSAIDs (e.g., ibuprofen, naproxen) can trigger or worsen flare-ups. Discuss pain relief options with your doctor.
Smoking Cessation: While the relationship between smoking and IBD is complex (smoking is a risk factor for Crohn’s but might paradoxically affect UC), quitting smoking is always recommended for overall health and can reduce inflammation pathways.
Regular Monitoring: Adhering to scheduled doctor appointments, follow-up tests (blood work, stool tests, colonoscopies), and open communication with your healthcare team is vital to monitor disease activity and adjust uc treatment proactively.
4.3. Lifestyle Adjustments
Beyond specific medical management, adopting a healthy lifestyle can contribute to overall well-being and potentially reduce the burden of ulcerative colitis:
Regular Exercise: Can help manage stress, improve mood, and potentially reduce inflammation, though exercise intensity may need adjustment during flares.
Adequate Sleep: Prioritizing consistent and sufficient sleep supports immune function and overall physical and mental health.
4.4. Expert Insight: Diet as a Trigger, Not a Cure
Expert Insight: A common myth is that “if I follow a perfect diet, I can cure my ulcerative colitis or completely prevent all flare-ups.” While dietary management is a crucial part of living with UC, medical experts emphasize the fact that UC is a complex chronic autoimmune disease. Dietary changes can significantly help manage symptoms, reduce inflammation, and identify individual triggers, but they do not guarantee complete prevention of flares, nor do they replace necessary medical treatment. Relying solely on diet without appropriate medication can lead to disease progression and severe complications.
5. What Are the Treatment and Management Options for Ulcerative Colitis?
Ulcerative colitis treatments focus on two primary goals: inducing remission (stopping a flare-up) and maintaining remission (preventing future flare-ups), ultimately improving an individual’s quality of life. For those asking “is ulcerative colitis curable?” or seeking a “permanent cure for ulcerative colitis,” it’s important to understand that currently, there is no definitive permanent cure, but long-term remission is achievable with effective management. The range of treatments for ulcerative colitis is broad and highly individualized.
5.1. Goals of UC Treatment
The overarching goals of ulcerative colitis treatment and management include:
Induce Remission: To stop active inflammation and alleviate acute ulcerative colitis symptoms.
Maintain Remission: To prevent future flare-ups and sustain periods of minimal or no symptoms.
Heal Mucosal Inflammation: To reduce inflammation and promote healing of the colon lining.
Prevent Complications: To minimize the risk of complications suchs as colon cancer, strictures, or perforations.
Improve Quality of Life: To enable individuals to live a full, active life with minimal disruption from their condition.
5.2. Medical Treatments (Medications)
Medicine for ulcerative colitis is the primary approach to controlling inflammation. The choice of ulcerative colitis medications depends on the severity and extent of the disease.
Aminosalicylates (5-ASAs): These are often the first-line medication for ulcerative colitis for mild to moderate UC, particularly for maintaining remission. They work by reducing inflammation in the lining of the colon. Examples include mesalamine, sulfasalazine, balsalazide, and olsalazine. They can be taken orally or topically (as suppositories or enemas for rectal/left-sided disease).
Corticosteroids: Drugs like prednisone or budesonide are powerful anti-inflammatory agents used for short-term control of moderate to severe flare-ups. They are highly effective at inducing remission quickly but are not used for long-term maintenance due to significant side effects.
Immunomodulators: These drugs for ulcerative colitis work by suppressing the immune system to reduce inflammation. They are used for individuals who don’t respond to 5-ASAs or need to reduce steroid dependence. Examples include azathioprine, 6-mercaptopurine, and methotrexate.
Biologic and Biosimilar Therapies: These are targeted therapies administered by injection or infusion for moderate to severe ulcerative colitis that hasn’t responded to conventional uc treatments. They work by blocking specific proteins in the immune system that cause inflammation. Examples include anti-TNF agents (e.g., infliximab, adalimumab), anti-integrins (e.g., vedolizumab), and anti-IL-12/23 (e.g., ustekinumab).
Janus Kinase (JAK) Inhibitors: These are newer oral medications (e.g., tofacitinib, upadacitinib) that target specific pathways within immune cells to reduce inflammation. They represent a significant advance in uc treatments for moderate to severe UC.
5.3. Surgical Treatments
When medical ulcerative colitis treatments fail to control the disease, or if severe complications arise, surgery may become a necessary option.
Colectomy: The most common surgical procedure for ulcerative colitis is the removal of the entire colon and rectum (total proctocolectomy). This procedure effectively “cures” the inflammation in the colon because the diseased organ is removed.
Ileal Pouch-Anal Anastomosis (IPAA or J-pouch surgery): After colectomy, surgeons can create an internal pouch from the small intestine and connect it to the anus, allowing for bowel movements through the natural route.
Permanent Ileostomy: In some cases, a permanent opening (stoma) in the abdomen is created, to which the small intestine is attached, and waste collects in an external pouch.
While surgery to remove the colon can eliminate the inflammatory disease in the colon itself, it involves significant changes and potential long-term complications.
5.4. Lifestyle and Complementary Therapies
Complementary approaches can support medical ulcerative colitis therapy and enhance overall well-being:
Dietary Modifications: While no universal “UC diet” exists, identifying personal trigger foods through a food diary can help. Some individuals find relief with low-residue or low-FODMAP diets, especially during flares, to reduce symptoms like bloating and gas.
Stress Management: As stress can trigger flares, techniques like meditation, yoga, mindfulness, and counseling can help manage stress levels.
Probiotics: Research on probiotics for UC is ongoing. While some individuals report benefits, scientific evidence is still limited, and they should only be used after discussion with a healthcare provider.
5.5. Expert Insight: Adherence is Key to Remission
Expert Insight: A common myth is that “if my ulcerative colitis symptoms go away, I can stop taking my medication because I’m cured.” Leading gastroenterologists emphasize the crucial fact that UC medications are vital for maintaining remission and preventing future flares and serious complications, even when you feel well. Stopping medication without strict medical guidance can lead to severe relapses, disease progression, and a reduced chance of achieving long-term remission, making adherence to your prescribed regimen paramount for managing this chronic illness.
If you have questions about your ulcerative colitis treatment plan, are experiencing a flare-up, or need to discuss management options, MaNaDr offers a discreet and convenient platform to connect with online doctors 24/7 for expert consultations and personalized guidance.
6. How Is Ulcerative Colitis Diagnosed?
Receiving an accurate ulcerative colitis diagnosis can sometimes be a lengthy process due to the overlap of uc symptoms with other gastrointestinal conditions. Understanding how is ulcerative colitis diagnosed is crucial for patients seeking clarity and effective uc treatment.
6.1. Initial Assessment and Symptom Evaluation
The diagnostic process typically begins with a thorough evaluation by a healthcare professional, usually a gastroenterologist.
Medical History: The doctor will ask detailed questions about your symptoms of colitis, including the frequency and nature of bowel movements (colitis poop, ulcerative colitis stool), abdominal pain, bleeding, fatigue, and any family history of IBD. This helps distinguish it from other conditions like cholidis disease (Crohn’s disease) or IBS.
Physical Exam: A physical examination may reveal tenderness in the abdomen, signs of dehydration, or fever.
6.2. Diagnostic Tests
Several tests are used to confirm ulcerative colitis diagnosis, assess the extent of inflammation, and rule out other conditions.
Blood Tests:
Inflammation Markers: Tests like C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) can indicate inflammation in the body.
Anemia: Check for iron-deficiency anemia due to blood loss.
Nutritional Deficiencies: Assess levels of vitamins and minerals.
Stool Tests:
Infection Screening: To rule out bacterial or parasitic infections that can cause similar symptoms of colitis.
Fecal Calprotectin: A marker for intestinal inflammation that can indicate the need for further endoscopic investigation.
Endoscopy (Colonoscopy with Biopsy): This is considered the gold standard for ulcerative colitis diagnosis.
A flexible tube with a camera is inserted through the rectum to visualize the entire colon lining.
The doctor can directly observe the pattern of inflammation, which in UC is typically continuous, starting from the rectum and extending upwards.
Biopsies: Small tissue samples are taken from the inflamed areas. These samples are then examined under a microscope by a pathologist to confirm the presence of chronic inflammation and other characteristic changes of ulcerative colitis, and to differentiate it from other conditions like Crohn’s disease or microscopic colitis. This is how you confirm ulcerative colitis ulcers.
Imaging Tests:
CT Scan or MRI: Used to assess the extent of inflammation, identify complications (like perforations or abscesses), or evaluate areas that cannot be reached by a colonoscope.
CT Enterography/MR Enterography: Specifically used to visualize the small bowel, which is typically not affected by UC but can be involved in Crohn’s disease, helping in differentiation.
6.3. Differentiating from Other Conditions
It is crucial to differentiate ulcerative colitis from other conditions that cause similar colitis signs and symptoms:
Crohn’s Disease: Another major type of IBD. While both involve chronic inflammation, Crohn’s can affect any part of the digestive tract (from mouth to anus) and cause patchy, “skip” lesions, while UC is limited to the colon and rectum with continuous inflammation.
Irritable Bowel Syndrome (IBS): IBS causes abdominal pain and changes in bowel habits, but it does not involve inflammation or damage to the bowel, unlike UC.
Infections: Bacterial or parasitic infections can cause acute colitis symptoms, but these are typically temporary and resolve with treatment, unlike the chronic nature of UC.
6.4. Expert Insight: The Diagnostic Imperative
Expert Insight: A common myth is that “a simple blood test or stool test can definitively diagnose ulcerative colitis, making invasive procedures unnecessary.” While blood and stool tests can indicate inflammation and help rule out infections, leading gastroenterological associations emphasize the crucial fact that a definitive diagnosis of ulcerative colitis primarily relies on a colonoscopy with biopsies. This allows for direct visualization of the colon lining and microscopic confirmation of the characteristic chronic inflammation and ulcers, which is essential to differentiate UC from other bowel conditions and guide appropriate long-term treatment.
If you are experiencing persistent digestive symptoms and wondering how is ulcerative colitis diagnosed or need to discuss potential tests, MaNaDr offers a convenient platform for initial symptom discussion before seeing a specialist, or to help you understand complex test results.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified healthcare professional for diagnosis and treatment of any medical condition.